
Overview
Wegovy (semaglutide) is a long‑acting GLP‑1 receptor agonist available as a once‑weekly subcutaneous injection and a once‑daily high‑dose oral tablet. It is approved to reduce major adverse cardiovascular events in adults with established cardiovascular disease and obesity or overweight, to support long‑term weight management in adults and adolescents with obesity or adults with overweight plus comorbidities, and to treat noncirrhotic MASH with moderate to advanced fibrosis in adults under an accelerated approval pathway. The current U.S. prescribing information, revised in December 2025, integrates these indications for both injection and tablet formulations, while incorporating updated guidance on severe gastrointestinal events, acute kidney injury, and peri‑procedural aspiration risk.
The clinical relevance of Wegovy reflects the convergence of three high‑burden conditions—obesity, cardiovascular disease, and metabolic liver disease—where weight reduction and metabolic improvement can modify long‑term outcomes but where durable, non‑surgical options have historically been limited. The SELECT, STEP, and ESSENCE programs collectively support its role across this spectrum, with robust efficacy but a characteristic GLP‑1 RA tolerability profile that necessitates careful initiation, titration, and monitoring.
Also Read: How to choose the Best cough syrup in India (2026 Guide)
Disease background & treatment landscape
Obesity and overweight affect roughly 70% of U.S. adults and are major contributors to type 2 diabetes, cardiovascular disease, and certain cancers, driving substantial morbidity, mortality, and healthcare expenditures. Even a 5–10% reduction in body weight is associated with meaningful reductions in cardiometabolic risk, yet lifestyle interventions alone often fail to achieve or sustain this level of loss in real‑world settings. Pharmacologic options historically produced modest weight loss, were limited by tolerability or safety concerns, and rarely demonstrated improvement in hard cardiovascular endpoints.
Cardiovascular disease remains the leading cause of death among people with obesity, with overlapping drivers including insulin resistance, dyslipidemia, inflammation, sleep apnea, and hemodynamic load. Prior to SELECT, no weight‑management medication carried a specific indication to lower MACE risk in patients with overweight or obesity but without diabetes. The SELECT findings therefore inform a new paradigm in which obesity pharmacotherapy can be deployed explicitly for secondary cardiovascular prevention.
Metabolic dysfunction‑associated steatohepatitis (MASH), previously termed NASH, affects an estimated 6% of U.S. adults and is tightly linked to obesity, insulin resistance, and cardiometabolic disease. Progression to advanced fibrosis and cirrhosis leads to liver‑related morbidity and mortality, while competing CV risk remains high. Until Wegovy’s MASH indication, patients with F2–F3 fibrosis lacked any FDA‑approved pharmacologic therapy targeting steatohepatitis resolution and fibrosis improvement, relying primarily on lifestyle modification and bariatric surgery.
Against this background, semaglutide’s ability to deliver sustained double‑digit percentage weight loss, improve cardiometabolic markers, reduce MACE, and favorably modify histologic endpoints in MASH positions Wegovy as a versatile agent across cardiometabolic care pathways, provided its risks and limitations are fully understood and respected.

Mechanism of action
Semaglutide is a GLP‑1 analogue with 94% sequence homology to human GLP‑1 that selectively activates GLP‑1 receptors, the same receptors engaged by endogenous GLP‑1 secreted from intestinal L‑cells in response to nutrient ingestion. In the pancreas, GLP‑1 receptor activation augments glucose‑dependent insulin secretion and suppresses inappropriate glucagon secretion, thereby improving post‑prandial glycemia without a high intrinsic risk of hypoglycemia in the absence of concomitant insulin or secretagogues. In the gastrointestinal tract, delayed gastric emptying slows nutrient delivery and contributes to early satiety, while central actions on GLP‑1 receptor–positive neurons in the hypothalamus and brainstem reduce hunger and alter reward‑related eating behavior.
The chronic negative energy balance induced by semaglutide leads to sustained reductions in body weight, preferentially reducing fat mass with relative preservation of lean mass compared with non‑pharmacologic weight loss alone. Weight loss in turn improves blood pressure, lipid profile, insulin sensitivity, and systemic inflammatory markers, mechanisms that likely contribute to the 20% relative reduction in MACE observed in the SELECT trial despite the absence of diabetes in the enrolled population.
In the liver, weight loss and improved insulin sensitivity reduce hepatocellular fat accumulation and inflammatory signaling, key drivers of MASH pathogenesis. ESSENCE data suggest that Wegovy’s impact on histologic endpoints—resolution of steatohepatitis without fibrosis worsening and ≥1‑stage fibrosis improvement without MASH worsening—may be mediated through these pathways and possibly direct GLP‑1 receptor–related effects, although the exact mechanistic contribution beyond weight loss remains an area of active research.
From a practical standpoint, Wegovy can be conceptualized as a pharmacologic amplifier of lifestyle interventions: by reducing appetite, slowing gastric transit, and improving satiety signals, it increases the probability that patients can adhere to and sustain calorie restriction and activity goals that would otherwise be difficult to maintain long‑term.
Clinical evidence
SELECT – cardiovascular outcomes
SELECT enrolled 17,604 adults aged ≥45 years with established atherosclerotic cardiovascular disease (prior MI, stroke, or symptomatic peripheral arterial disease) and BMI ≥27 kg/m², but without diabetes, randomizing them 1:1 to semaglutide 2.4 mg SC weekly (after titration) or placebo on top of standard CV therapies. The median follow‑up was approximately 39–40 months, and the primary endpoint was time to first MACE (CV death, non‑fatal MI, or non‑fatal stroke).
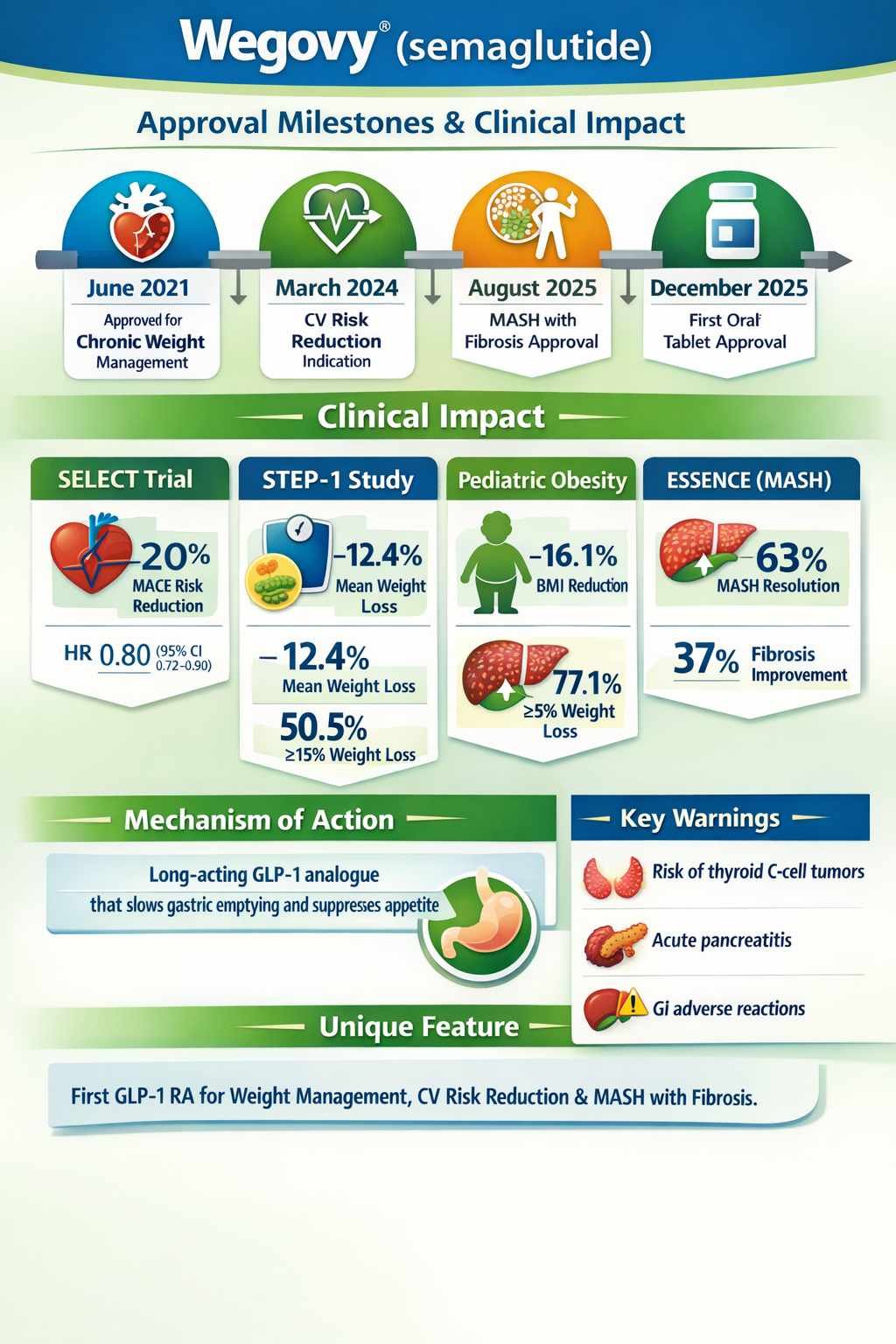
Wegovy reduced the risk of MACE with a hazard ratio of 0.80 (95% CI 0.72–0.90; p<0.001), corresponding to 6.5% vs 8.0% event rates in the semaglutide and placebo arms, respectively, and an absolute risk reduction around 1.5 percentage points. All three components of the composite endpoint contributed to the observed benefit. Subgroup analyses indicated consistent relative risk reductions across baseline BMI categories, sex, and HbA1c strata, suggesting that the CV benefit is not confined to specific subgroups within the obesity population.
Importantly, semaglutide‑treated patients experienced sustained weight loss (mean ~10.2% vs 1.5% at 208 weeks) and improvements in waist circumference and waist‑to‑height ratio, anthropometric changes that track with cardiometabolic risk reduction. While the trial was not designed to formally disentangle weight loss–mediated vs weight‑independent mechanisms, the magnitude and durability of weight loss likely play a substantial role in risk modification.
Clinicians should note that in SELECT, treatment discontinuation due to adverse events was 16% on semaglutide vs 8% on placebo, largely driven by GI events. Thus, for cardiologists and internists considering Wegovy primarily for CV risk reduction, careful titration, monitoring, and collaboration with endocrinology/obesity medicine can help balance tolerability with long‑term adherence.
STEP‑like adult weight‑management trials
In STEP‑1, 1,961 adults with obesity or overweight plus comorbidity but without diabetes were randomized 2:1 to semaglutide 2.4 mg weekly vs placebo plus lifestyle intervention for 68 weeks. The coprimary endpoints—percent change in body weight and proportion achieving ≥5% weight loss—were both met with high statistical significance. Mean weight change was −14.9% vs −2.4% (ETD −12.4 percentage points; 95% CI −13.4 to −11.5; p<0.001), and 86.4% vs 31.5% achieved ≥5% weight loss, with more than half of semaglutide‑treated participants achieving ≥15% loss. Cardiometabolic markers and patient‑reported physical functioning improved in parallel.
STEP‑2 and related trials in adults with type 2 diabetes and overweight/obesity demonstrated somewhat smaller absolute weight reductions (e.g., ~9.6% vs 3.4% at 68 weeks; ETD −6.2 percentage points; 95% CI −7.3 to −5.2; p<0.0001), consistent with the more resistant weight‑loss phenotype in diabetes but still clinically meaningful. Across adult STEP trials, semaglutide’s impact on blood pressure, lipids, and glycemic parameters suggests broad metabolic benefits beyond weight alone.
Longer‑term data from STEP‑5 showed that a ~15% mean weight loss with semaglutide 2.4 mg could be maintained over two years, contrasting with typical weight regain patterns after diet‑only interventions. However, discontinuation of semaglutide in extension studies was associated with partial weight regain, underscoring the chronic nature of obesity and the likely need for ongoing pharmacotherapy to sustain benefits.
Pediatric obesity trial
The pediatric trial enrolled 201 adolescents aged 12–<18 years with BMI ≥95th percentile, randomizing them to semaglutide 2.4 mg weekly or placebo plus lifestyle over 68 weeks. Wegovy produced a −16.1% mean BMI change vs +0.6% with placebo, with an ETD of −16.7 percentage points (95% CI −20.3 to −13.2; p<0.0001), and 77.1% vs 19.7% achieved ≥5% BMI reduction. Adverse reactions were broadly similar to adults but with a higher incidence of gallbladder events, emphasizing the need for targeted counseling and monitoring in adolescents.
ESSENCE – MASH with F2–F3 fibrosis
ESSENCE studied adults with biopsy‑confirmed MASH and F2–F3 fibrosis, randomizing them to semaglutide 2.4 mg or placebo with an initial analysis at week 72 and planned continuation to week 240 for clinical outcomes. At week 72, 63% of Wegovy vs 34% of placebo patients achieved resolution of steatohepatitis without worsening fibrosis (difference 29 percentage points; 95% CI 21–36), while 37% vs 22% achieved ≥1‑stage fibrosis improvement without worsening MASH (difference 14 percentage points; 95% CI 8–21).
These biopsy‑based endpoints supported accelerated approval for the MASH indication, but clinical benefit in terms of liver‑related outcomes (decompensation, transplant, mortality) remains to be fully demonstrated; ongoing follow‑up will determine whether histologic gains translate into long‑term clinical advantage. Until those data mature, clinicians should frame Wegovy’s MASH indication as evidence‑supported for histologic response but still under confirmatory evaluation for hard liver outcomes.
Safety profile and risk management
Safety considerations for Wegovy are dominated by its GLP‑1 class effects and includes both common, generally manageable GI symptoms and less frequent but clinically significant risks.
The boxed warning for thyroid C‑cell tumors is based on rodent carcinogenicity studies showing dose‑ and duration‑dependent C‑cell tumor formation at exposures relevant to human dosing; the human relevance remains uncertain, but contraindications in MTC and MEN 2 and counseling on thyroid mass symptoms are mandatory. Post‑marketing surveillance, including dedicated analyses for MTC signals, is ongoing.
Gastrointestinal events—nausea, vomiting, diarrhea, constipation, abdominal pain—are the most frequently reported adverse reactions and the leading cause of treatment discontinuation. In adult weight‑management trials, 4.1% of injection‑treated and 2% of tablet‑treated patients experienced severe GI adverse reactions vs 0.9% and 0% with placebo, respectively. Careful dose escalation, patient education (e.g., smaller meals, slower eating, avoiding high‑fat foods during titration), and proactive management of nausea and constipation can mitigate these effects and support adherence.
Semaglutide is associated with a modest increase in gallbladder disease risk beyond that attributable to weight loss alone, with cholelithiasis reported in 1.6–2.5% vs 0.7–1.0% and cholecystitis in 0.6% vs 0.2% of Wegovy vs placebo‑treated adults in weight‑management trials, and higher rates in adolescents. Clinicians should maintain a low threshold for evaluating biliary symptoms and consider the potential benefit–risk of continuing therapy in patients with recurrent gallstone disease.
Acute pancreatitis has been observed with GLP‑1 RAs, and Wegovy trials reported rare adjudicated cases (about 0.2 vs <0.1 cases per 100 patient‑years in adults), necessitating prompt drug discontinuation and work‑up in patients with severe, persistent abdominal pain. Acute kidney injury, often in the context of GI fluid losses, underscores the importance of hydration counseling and renal function monitoring in susceptible patients, particularly during dose escalation.
Other notable risks include diabetic retinopathy complications—seen previously with lower‑dose injectable semaglutide in high‑risk type 2 diabetes cohorts—and modest increases in resting heart rate. Patients with pre‑existing diabetic retinopathy should have regular ophthalmologic follow‑up, and any visual changes warrant prompt evaluation.
Suicidal ideation and behavior have been observed with other weight‑management agents, and Wegovy carries a class‑consistent warning; patients should be screened for mood disorders, monitored for emerging depressive symptoms or suicidal thoughts, and the drug avoided in individuals with a history of suicide attempts or active suicidal ideation.
Finally, delayed gastric emptying raises peri‑anesthetic aspiration concerns. The label notes rare reports of pulmonary aspiration during general anesthesia or deep sedation among patients on GLP‑1 RAs despite adherence to standard fasting protocols, but available data are insufficient to define specific peri‑procedural holding strategies. Until guidance evolves, coordination between prescribing clinicians and anesthesiologists is advisable for patients scheduled for procedures.
Dosing and practical use
In practice, semaglutide initiation requires clear communication about goals, titration schedules, expected side effects, and the need for sustained lifestyle modification. For both injection and tablet formulations, a gradual dose‑escalation schedule over approximately 16 weeks (injection) or 90 days (tablets) is standard to improve GI tolerability.
For prescribers, key considerations include:
- Confirming that the intended use is FDA‑approved (CV risk reduction, chronic weight management, or adult MASH with F2–F3 fibrosis) and that BMI and comorbidity criteria are met.
- Excluding contraindications (MTC/MEN 2, prior anaphylaxis/angioedema to semaglutide) and identifying risk factors such as prior pancreatitis, gallbladder disease, severe GI motility disorders, and advanced diabetic retinopathy.
- Establishing realistic expectations around weight‑loss magnitude, time to benefit, and chronic nature of therapy, particularly regarding potential weight regain after discontinuation.
- Integrating Wegovy with background therapies (antihypertensives, statins, antiplatelets) and adjusting doses of insulin or sulfonylureas when needed to reduce hypoglycemia risk.
For pharmacists, responsibilities include ensuring appropriate product selection (pen vs tablet; strength and titration pack), verifying that patients are not co‑dispensed other semaglutide‑containing products or GLP‑1 RAs, and counseling on administration specifics—especially the need to take tablets with water only and delay other oral medications by at least 30 minutes. Monitoring for potential drug–drug interactions due to delayed gastric emptying is also critical, particularly for narrow‑therapeutic‑index agents.
For nurses and allied HCPs, education on injection technique, rotation of sites, recognition of GI and gallbladder symptoms, and reinforcement of lifestyle interventions are central. They also play a key role in identifying mood changes, visual symptoms, or signs of dehydration that should trigger prescriber review.
Patient‑centered considerations
Eligibility and benefit must be weighed against individual comorbidities, preferences, and treatment burden. Wegovy may be particularly suitable for:
- Adults with obesity or overweight and established CV disease in whom additional CV risk reduction beyond optimal medical therapy is a priority.
- Patients with severe obesity and multiple weight‑related comorbidities who have not achieved sufficient weight loss with lifestyle measures alone and either are poor candidates for bariatric surgery or prefer pharmacologic options.
- Adults with noncirrhotic MASH and F2–F3 fibrosis where histologic improvement could delay or prevent progression, pending confirmatory outcome data.
Treatment burden includes weekly injections or daily tablets, frequent early‑phase contact for titration and side‑effect management, and potential insurance hurdles and out‑of‑pocket costs. However, for many patients, weight loss–associated improvements in mobility, sleep apnea, glycemic control, and quality of life can be substantial, typically emerging over weeks to months of therapy.
Shared decision‑making is essential in scenarios such as borderline BMI thresholds, older age with frailty, complex polypharmacy, or psychiatric comorbidity, where benefit–risk calculus is individualized.
Regulatory & post‑marketing journey
Wegovy’s regulatory trajectory began with its 2021 approval for chronic weight management in adults with obesity or overweight plus comorbidity, following the STEP program. Subsequent supplements added adolescent obesity (≥12 years), refined titration guidance, and updated safety sections as more post‑marketing data accrued.
In March 2024, FDA approved a new indication to reduce MACE in adults with established CV disease and overweight/obesity based on SELECT, marking the first obesity medication with a dedicated CV risk‑reduction label in this population. In August 2025, accelerated approval was granted for treating noncirrhotic MASH with F2–F3 fibrosis, contingent on confirmatory ESSENCE outcomes. In December 2025, the Wegovy 25 mg oral tablet formulation was approved for adult weight management and CV risk reduction, using OASIS‑4 and SELECT as key evidence.
Post‑marketing commitments include ongoing MASH outcome analyses, cardiovascular sub‑studies, and continued pharmacovigilance for signals such as MTC, pancreatitis, severe GI events, renal injury, and aspiration events under anesthesia. Label updates in 2024–2025 expanded Warnings and Precautions for acute kidney injury due to volume depletion, severe GI adverse reactions, and peri‑procedural aspiration risk, reflecting evolving safety understanding.
Conclusion & forward look
Wegovy represents a comprehensive GLP‑1 RA platform addressing chronic weight management, secondary cardiovascular prevention, and histologic improvement in MASH with fibrosis within a single semaglutide backbone and shared titration logic. Across SELECT, STEP‑like trials, pediatric obesity studies, and ESSENCE, Wegovy demonstrates robust, durable weight loss, clinically meaningful CV risk reduction, and promising liver histologic responses, albeit with an established GI‑dominant tolerability profile and specific but manageable safety concerns.
In clinical practice, Wegovy’s place in therapy is likely as:
- A foundational pharmacologic option for patients with obesity or overweight and established cardiovascular disease who remain at high residual risk despite standard therapies.
- A long‑term weight‑management agent for selected adults and adolescents where lifestyle measures alone are insufficient and where the benefits of substantial, sustained weight loss outweigh risks.
- A targeted therapy for adults with noncirrhotic MASH and F2–F3 fibrosis in whom histologic improvement is desired and who can be closely monitored pending outcome data.
Key unknowns include the durability of MACE benefits in broader populations, the long‑term clinical impact of histologic MASH improvements, the optimal duration of therapy, and comparative effectiveness versus emerging incretin‑based agents. As additional data and competing therapies emerge, treatment algorithms will continue to evolve, but Wegovy’s current evidence base positions it as a central, though not universal, tool in contemporary cardiometabolic and liver‑disease management.
Disclaimer: This article is for informational purposes only and does not replace the full Prescribing Information or professional medical advice.
References:
- Wegovy® (semaglutide) injection and tablets – Prescribing Information. Novo Nordisk A/S. Updated December 2025. Available at: https://www.novo-pi.com/wegovy.pdf [accessed March 2026].
- Wegovy® (semaglutide) – Prescribing Information and Medication Guide. Novo Nordisk A/S. Available at: https://www.wegovy.com/prescribing-information.html [accessed March 2026].
- Wegovy (semaglutide) injection – US prescribing information, NDA 215256. Center for Drug Evaluation and Research (CDER), U.S. Food and Drug Administration. 2023 label revision. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215256s007lbl.pdf [accessed March 2026].
- Wilding JPH, Batterham RL, Calanna S, et al; STEP 1 Investigators. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989–1002. doi:10.1056/NEJMoa2032183.
- Semaglutide Treatment Effect in People With Obesity (STEP 1). American College of Cardiology Clinical Trials Summary. 2021. Available at: https://www.acc.org/latest-in-cardiology/clinical-trials/2021/02/18/19/23/step-1 [accessed March 2026].
- STEP 1: Research Study Investigating How Well Semaglutide Works in People Suffering From Overweight or Obesity (NCT03548935). ClinicalTrials.gov. Updated 2021 Nov 19. Available at: https://clinicaltrials.gov/study/NCT03548935 [accessed March 2026].
- Lincoff AM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023. PubMed ID: 37952131. Available at: https://pubmed.ncbi.nlm.nih.gov/37952131/ [accessed March 2026].
- Semaglutide Effects on Cardiovascular Outcomes in People With Overweight or Obesity (SELECT). American College of Cardiology Clinical Trials Summary. 2023. Available at: https://www.acc.org/latest-in-cardiology/clinical-trials/2023/11/09/15/04/select [accessed March 2026].
- vvSELECT Trial: Semaglutide and cardiovascular outcomes in obesity without diabetes. CardioNerds. 2023. Available at: https://www.cardionerds.com/cardsjc-semaglutide-and-cardiovascular-outcomes-in-obesity-without-diabetes-select-trial/ [accessed March 2026].
- The SELECT Trial: A Brief Summary. Cleveland Clinic Podcast (Cardiac Consult). 2023. Available at: https://my.clevelandclinic.org/podcasts/cardiac-consult/the-select-trial-a-brief-summary [accessed March 2026].
- Once-weekly semaglutide in adolescents with obesity. N Engl J Med. 2022;387:2245–2257 (article PDF hosted at Lone Star Centers). Available at: https://lonestarcenters.com/wp-content/uploads/2025/11/once-weekly-semaglutide.pdf [accessed March 2026].
- Semaglutide once weekly helps adolescents lose weight (POEMs summary). Am Fam Physician. 2023 Jul 14. Available at: https://www.aafp.org/pubs/afp/issues/2023/0700/poems-semaglutide-weight-loss.html [accessed March 2026].
- Pediatric obesity research update: Once-weekly semaglutide in adolescents with obesity (STEP TEENS). Obesity Medicine Association Blog. 2024. Available at: https://obesitymedicine.org/blog/pediatric-obesity-research-update-once-weekly-semaglutide-in-adolescents-with-obesity/ [accessed March 2026].
- ESSENCE phase 3 trial of semaglutide showed significant improvements at 72 weeks in adults with MASH. Novo Nordisk press release. PR Newswire. 2025 Apr 30. Available at: https://www.prnewswire.com/news-releases/essence-phase-3-trial-of-semaglutide-showed-significant-improvements-at-72-weeks-in-adults-with-mash-published-in-nejm-301434567.html [accessed March 2026].
- ESSENCE phase 3 trial of semaglutide showed significant improvements at 72 weeks in adults with MASH. Yahoo Finance reprint. 2025 Apr 30. Available at: https://finance.yahoo.com/news/essence-phase-3-trial-semaglutide-213000752.html [accessed March 2026].
- Recent data from the ESSENCE trial on semaglutide in metabolic dysfunction–associated steatohepatitis. Gastroenterol Hepatol (N Y). 2024;20(XX):XX–XX. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11920021/ [accessed March 2026].
- Phase 3 ESSENCE trial: Semaglutide in metabolic dysfunction–associated steatohepatitis – secondary analyses. Novo Nordisk Science Hub (AASLD 2025 poster). 2025. Available at: https://sciencehub.novonordisk.com/content/dam/sciencehub/global/en/congresses-and-scientific-publications/congresses/aasld2025/ [accessed March 2026].
- Once-weekly semaglutide in adults with overweight or obesity (STEP 1) – structured abstract and commentary. Gastroenterology (GI.org Evidence-Based GI). 2024 Mar 5. Available at: https://gi.org/journals-publications/ebgi/once-weekly-semaglutide-in-adults-with-overweight-or-obesity/ [accessed March 2026].
- Reducing BMI below the obesity threshold in adolescents treated with once-weekly subcutaneous semaglutide 2.4 mg (STEP TEENS post hoc analysis). Obesity (Silver Spring). 2023;31(XX):XX–XX. Available at: https://onlinelibrary.wiley.com/doi/10.1002/oby.23808 [accessed March 2026].
- How much does Wegovy (semaglutide) cost without insurance? GoodRx Health. Updated 2024–2025. Available at: https://www.goodrx.com/wegovy/wegovy-for-weight-loss-cost-coverage [accessed March 2026].
- How much does Wegovy cost with GoodRx? GoodRx Help Center. 2025–2026. Available at: https://www.goodrx.com/answers/how-much-does-wegovy-cost-with-goodrx [accessed March 2026].
- Wegovy 2026 prices, coupons & savings tips. GoodRx Drug Prices. Updated 2026 Mar 23. Available at: https://www.goodrx.com/wegovy [accessed March 2026].
- Wegovy® cost and coverage information – “What to pay for Wegovy”. Novo Nordisk patient site. Updated 2026 Mar 19. Available at: https://www.wegovy.com/obesity/what-to-pay-for-wegovy.html [accessed March 2026].
- Prescribing Wegovy® pen or pill (HCP dosing and administration guide). Novo MedLink. Available at: https://www.novomedlink.com/obesity/products/treatments/wegovy/dosing-administration/prescribing-wegovy.html [accessed March 2026]

: A Potential Breakthrough in Diabetes Treatment")

